The basic urge to pee is surprisingly complex and can go awry as we age.
You’re driving somewhere, eyes on the road, when you start to feel a tingling sensation in your lower abdomen. That extra-large Coke you drank an hour ago has made its way through your kidneys into your bladder. “Time to pull over,” you think, scanning for an exit ramp.
To most people, pulling into a highway rest stop is a profoundly mundane experience. But not to neuroscientist Rita Valentino, who has studied how the brain senses, interprets, and acts on the bladder’s signals. She’s fascinated by the brain’s ability to take in sensations from the bladder, combine them with signals from outside of the body, like the sights and sounds of the road, then use that information to act—in this scenario, to find a safe, socially appropriate place to pee. “To me, it’s really an example of one of the beautiful things that the brain does,” she says.
Scientists used to think that our bladders were ruled by a relatively straightforward reflex—an “on-off” switch between storing urine and letting it go. “Now we realize it’s much more complex than that,” says Valentino, now director of the division of neuroscience and behavior at the National Institute of Drug Abuse. An intricate network of brain regions that contribute to functions like decision-making, social interactions, and awareness of our body’s internal state, also called interoception, participates in making the call.
In addition to being mind-bogglingly complex, the system is also delicate. Scientists estimate, for example, that more than 1 in 10 adults have overactive bladder syndrome—a common constellation of symptoms that includes urinary urgency (the sensation of needing to pee even when the bladder isn’t full), nocturia (the need for frequent nightly bathroom visits) and incontinence. Although existing treatments can improve symptoms for some, they don’t work for many people, says Martin Michel, a pharmacologist at Johannes Gutenberg University in Mainz, Germany, who researches therapies for bladder disorders. Developing better drugs has proven so challenging that all major pharmaceutical companies have abandoned the effort, he adds.
Recently, however, a surge of new research is opening the field to fresh hypotheses and treatment approaches. Although therapies for bladder disorders have historically focused on the bladder itself, the new studies point to the brain as another potential target, says Valentino. Combined with studies aimed at explaining why certain groups, such as post-menopausal women, are more prone to bladder problems, the research suggests that we shouldn’t simply accept symptoms like incontinence as inevitable, says Indira Mysorekar, a microbiologist at Baylor College of Medicine in Houston. We’re often told such problems are just part of getting old, particularly for women—“and that’s true to some extent,” she says. But many common issues are avoidable and can be treated successfully, she says: “We don’t have to live with pain or discomfort.”
A delicate balance
The human bladder is, at the most basic level, a stretchy bag. To fill to capacity—a volume of 400 to 500 milliliters (about 2 cups) of urine in most healthy adults—it must undergo one of the most extreme expansions of any organ in the human body, expanding roughly sixfold from its wrinkled, empty state.
To stretch that far, the smooth muscle wall that wraps around the bladder, called the detrusor, must relax. Simultaneously, sphincter muscles that surround the bladder’s lower opening, or urethra, must contract, in what scientists call the guarding reflex.
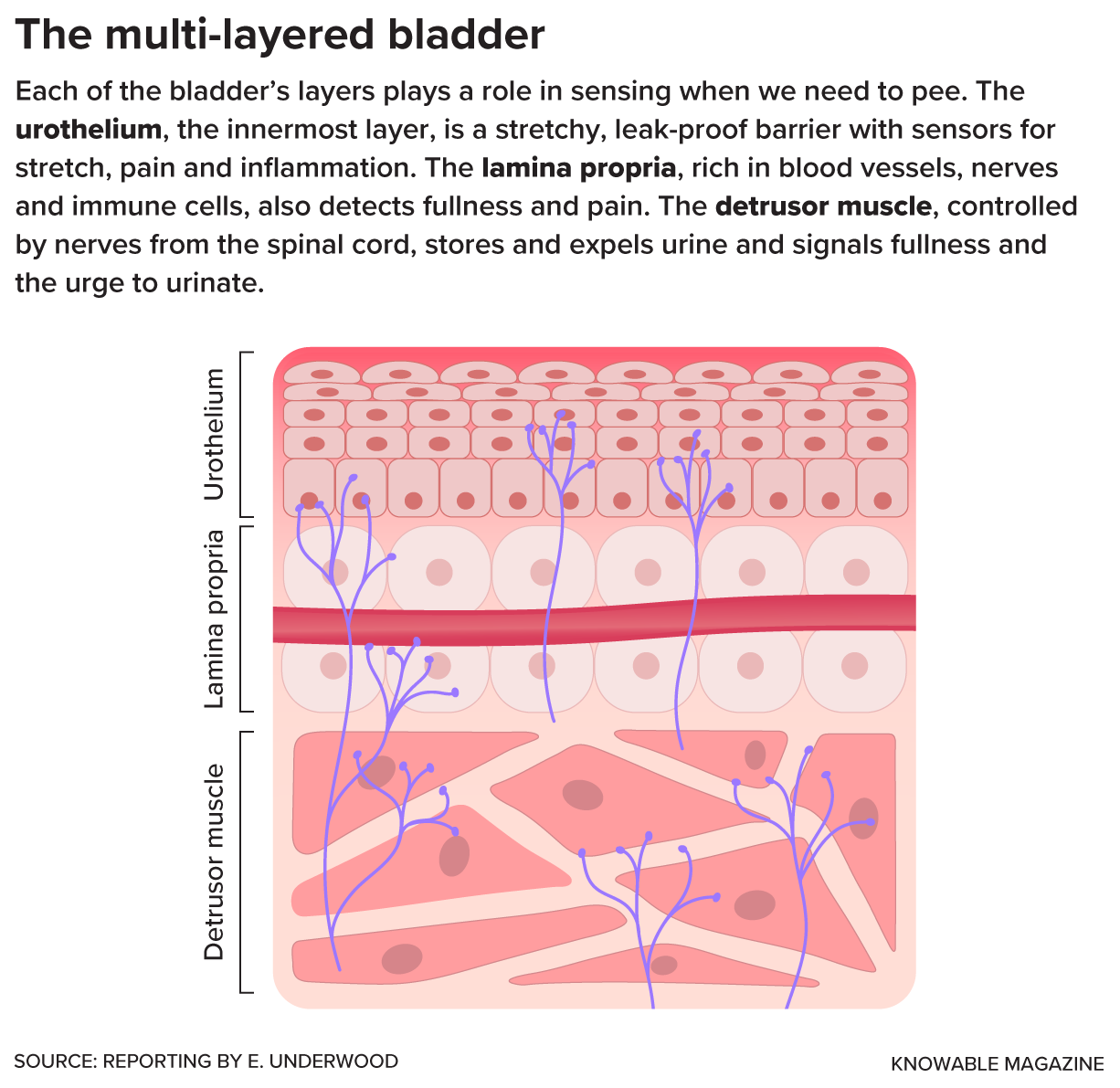
It’s not just sensory neurons (purple) that can detect stretch, pressure, pain and other
sensations in the bladder. Other types of cells, like the umbrella-shaped cells that form
the urothelium’s barrier against urine, can also sense and respond to mechanical forces
— for example, by releasing chemical signaling molecules such as adenosine triphosphate
(ATP) as the organ expands to fill with urine.
Knowable Magazine
Filling or full, the bladder spends more than 95 percent of its time in storage mode, allowing us to carry out our daily activities without leaks. At some point—ideally, when we decide it’s time to pee—the organ switches from storage to release mode. For this, the detrusor muscle must contract forcefully to expel urine, while the sphincter muscles surrounding the urethra simultaneously relax to let urine flow out.
For a century, physiologists have puzzled over how the body coordinates the switch between storage and release. In the 1920s, a surgeon named Frederick Barrington, of University College London, went looking for the on-off switch in the brainstem, the lowermost part of the brain that connects with the spinal cord.
Working with sedated cats, Barrington used an electrified needle to damage slightly different areas in the pons, part of the brainstem that handles vital functions like sleeping and breathing. When the cats recovered, Barrington noticed that some demonstrated a desire to urinate—by scratching, circling, or squatting—but were unable to voluntarily go. Meanwhile, cats with lesions in a different part of the pons seemed to have lost any awareness of the need to urinate, peeing at random times and appearing startled whenever it happened. Clearly, the pons served as an important command center for urinary function, telling the bladder when to release urine.
Beyond Barrington’s nucleus
Barrington’s work laid the foundation for our current understanding of the neural circuitry of bladder control. But we now know there’s much more than the pons involved.
As the bladder fills with urine, stretch-sensing cells in the detrusor, as well as in inner layers of the bladder wall, send signals of fullness up the spinal cord to a part of the brainstem called the periaqueductal gray. The signals then travel to a region called the insula, which acts as a kind of sensor: The fuller the bladder becomes, the more neurons in the insula fire off tiny electrical pulses called action potentials.
Next, a region of the brain that’s responsible for planning and making decisions—the prefrontal cortex—calculates whether it’s a socially acceptable moment to urinate. If the answer is yes, it sends a signal back to the periaqueductal gray, which in turn sends an all-clear signal to that part of the pons Barrington identified in cats—now aptly called Barrington’s nucleus. The signal goes back down to the bladder, and voila, urination occurs.
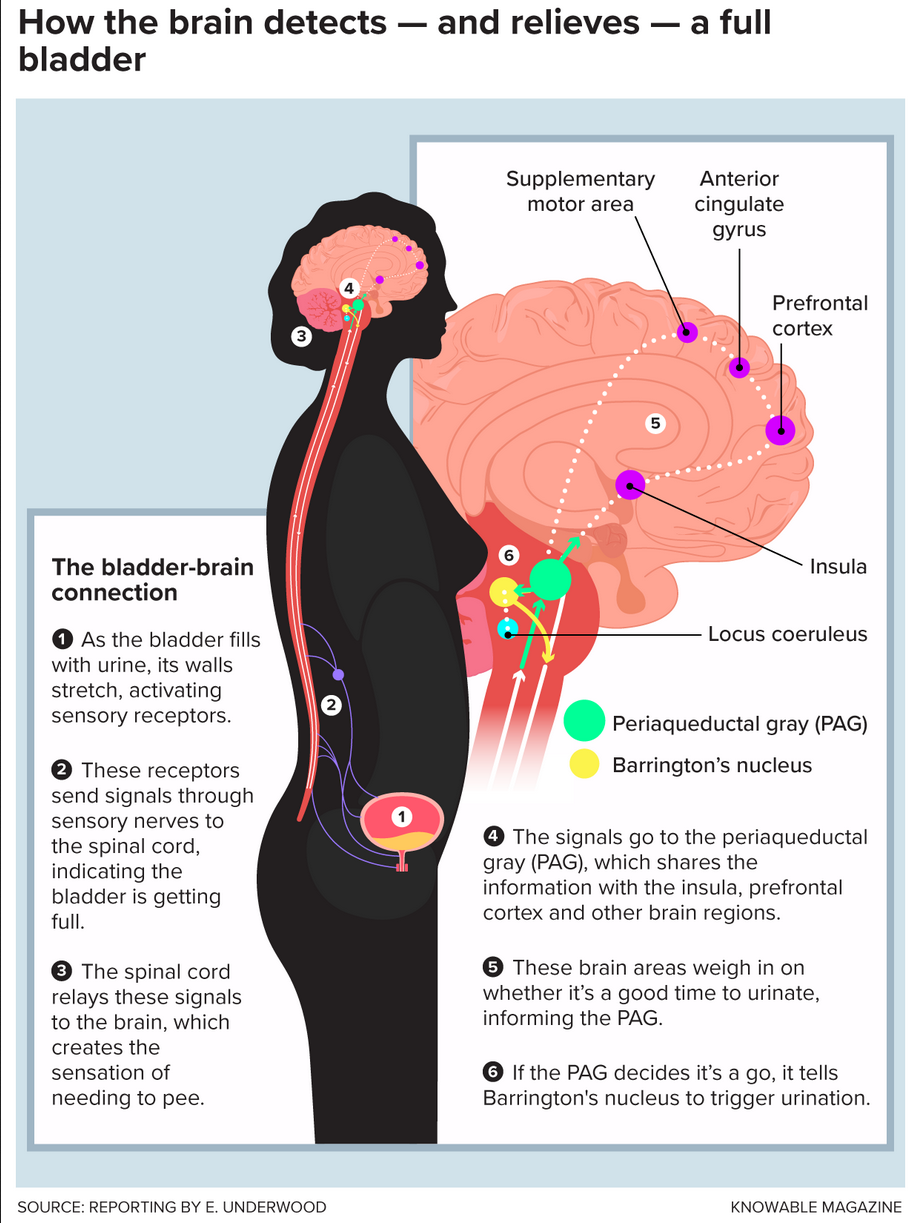
A simplified representation of some of the nerve pathways and
brain regions that allow most healthy people to detect when the
bladder is filling or full, predict how long they can wait to urinate,
and successfully carry out a plan to “hold it” or “go.” Disruptions
at any level of this complex, two-way system of neuronal
communication can lead to bladder disorders, as millions of people
worldwide know firsthand.
Knowable Magazine
Over the past decade, super-precise tools for mapping how different brain regions connect and interact have made the picture even more elaborate.
Valentino and her team have used a technique that can monitor and analyze the electrical activity of neurons across multiple sites within the brain simultaneously to show that neurons located in a part of the brainstem called the locus coeruleus start to fire in a steady, rhythmic pattern when the bladder reaches a certain level of fullness. Wavelike, this activity spreads to the brain’s outer layer, the cortex, and rouses the brain to a more alert state about 30 seconds before urination occurs. Valentino hopes that observations like this could inform treatments for common problems like nocturia and bedwetting, but they also may help to explain something basic that most people have encountered.
“I think that’s one of one of the major reasons you wake up when you have to urinate,” Valentino says. “The locus is saying, ‘Stop what you’re doing and focus on this.’”
Learning to hold it
Control over when and where we pee takes time to develop, as anyone who has potty-trained a toddler can attest. At birth, urination is governed not by the brain, but by a spinal reflex that springs into action when the bladder reaches a certain capacity. Only at around age 3 or 4 do the brain regions that govern functions like social awareness and decision-making override the reflex, says Hanneke Verstegen, a neuroscientist at Beth Israel Deaconess Medical Center and Harvard Medical School in Boston.
It’s not possible to watch how this process unfolds in the brainstems of human infants. But Verstegen and her colleagues are studying a similar process in baby lab mice, which gain voluntary control over urination by about three to five weeks. At that point, the baby mice start to pee in a designated corner—a behavior that’s not unlike that of toilet-trained toddlers, she says. Interestingly, the more primitive, automatic spinal reflex we have as infants never completely disappears: When a spinal cord injury damages the nerves that carry signals between the bladder and brain, the reflex can reemerge, often causing incontinence or other problems that require using a catheter.
Spinal cord injuries are just one of the many ways that brain-bladder communication can go awry. As the brain ages, the long, spindly neuronal projections that transmit messages in and between regions that control urination can also lose their integrity and derail normal bladder function—a process that’s often accelerated in Parkinson’s and Alzheimer’s disease.
Medical physicist Becky Clarkson of the University of Pittsburgh and her colleagues are using neuroimaging tools such as functional magnetic resonance imaging (fMRI), which looks at fluctuations in blood oxygen levels to indicate which parts of the brain are active, to understand how the elegant brain mechanisms governing urination break down. “We’re trying out work out what pathways maybe have damage,” she says. “How does the brain normally control the bladder? How does it fail to control the bladder?”
Most of the participants in Clarkson’s studies are women over 60, the group of people that has the highest rate of overactive bladder syndrome. Roughly 11 percent of the general population has overactive bladder, but more than 45 percent of post-menopausal women report symptoms.
Scientists aren’t sure what causes overactive bladder syndrome, or why it’s so common in older women. Some point to changes in the bladder itself. Mysorekar, for one, has found that during menopause, a proliferation of immune cells form tiny lumps resembling lymph nodes on the female bladder lining. These lesions increase the bladder’s sensitivity to even nominal levels of E. coli, the bacterium that causes most urinary tract infections, she says, causing chronic bladder pain or overactive bladder syndrome.
Another major contributor to overactive bladder syndrome in both women and men is detrusor overactivity—erratic contractions of the bladder muscle that send false signals of fullness to the brain. Nearly all existing treatments aim to quiet these spasms: The most prescribed class of medications, antimuscarinic drugs, blocks the activity of acetylcholine, a nerve-signaling chemical that triggers detrusor contractions, for example.
If medications don’t work, clinicians often recommend dosing the detrusor with shots of botulinum toxin, also known as Botox, so it doesn’t contract as much. Sometimes, they’ll also deliver electrical current to nerves in the spinal cord through a surgical implant or electrodes placed on the skin, attempting to restore normal activity in the spinal nerves that control the bladder muscle.
The problem with all these detrusor-taming treatments is that they can have unwanted side effects—including, in rare cases, impairing the ability to release urine, says Michel. “It’s a very thin line you’re walking—if you do too much, you can no longer expel; if you do too little, you have problems with storage.” Antimuscarinic drugs have been linked to symptoms of cognitive decline, particularly in older people, raising safety concerns. And not everyone with overactive bladder syndrome has an overactive detrusor muscle, prompting some scientists to ask if the problem for some patients lies elsewhere in the body, such as inside the brain.
Home safe
If you’ve ever come home after a long day at work, and—just as you unlocked the front door—felt a sudden, even overwhelming urge to go, you’ve experienced the tight link that scientists have long known exists between the brain and bladder. Called latchkey incontinence, this type of urge doesn’t have anything to do with how full your bladder is. (It’s also different from a physical inability to hold urine in when we sneeze, cough, or jump: That common problem, called stress incontinence, usually occurs due to weak pelvic floor muscles.)
Some scientists think that the urgent sensations that characterize overactive bladder syndrome may be conditioned responses like the ones that Russian physiologist Ivan Pavlov created in the 1890s when he trained dogs to associate food with the sound of a metronome. For some people, that conditioning could be years of waiting to get home to urinate so they can use their own bathrooms, Clarkson and her team hypothesize. For others, it might arise from a variety of situations and triggers, like the sound of running water. It’s normal if such intense sensations happen occasionally, but if they happen a lot, researchers consider it a potentially worrisome symptom.
Women with overactive bladders often have unusual patterns of brain activity, Clarkson and other groups have found. In a typical experiment in Clarkson’s lab, study participants lie flat in an fMRI machine while a catheter infuses fluid into the bladder until they say they are feeling full. A technician removes some fluid, then replaces it, repeating the process multiple times.
Using this approach, Clarkson and other researchers have built a model of how the brain controls the bladder, involving regions such as the insula, which processes fullness signals from the bladder, and the prefrontal cortex, which helps determine if it’s an appropriate time and place to pee. Two additional regions, the supplementary motor area and the anterior cingulate cortex, appear to work together to gauge just how urgent the need to urinate is and execute the pelvic floor muscle contractions that help us hold it until a bathroom is found. These areas tend to be more active in some people with overactive bladder syndrome, possibly contributing to the overwhelming sense of urgency even when their bladders are only partly full. “We think that’s almost like a panic station,” Clarkson says. “When you have urgency, you gotta go.”
A few years ago, one of Clarkson’s colleagues noted that the intense urges in overactive bladder syndrome are similar to the cravings former smokers feel in certain situations, like a bar where they used to smoke. Intrigued, Clarkson teamed up with smoking-cessation researcher Cynthia Conklin from the University of Pittsburgh, adapting a method from smoking studies to investigate how women with overactive bladder respond to personal triggers. The women were shown photographs of the places that triggered their own urgency, like their front doors or in one case, the entrance to a Target supermarket. Viewing these triggers increased activity in brain regions associated with attention, decision-making, and bladder control, compared to “safe” photos.
Certain behavioral therapies seem to help women with overactive bladder syndrome respond more calmly to their urgency triggers, Clarkson says. For example, her team’s preliminary data suggest that mindfulness techniques like a body-scan meditation, which prompts participants to relax from head to toe, can reduce the intensity of the bladder sensations. They also found that a noninvasive form of brain stimulation called transcranial direct current stimulation, or tDCS, could ease urgency.
Clarkson and her team have also explored how brain activity differs between women who do and don’t respond to treatment with botulinum toxin and pelvic floor muscle therapy, and they are currently investigating whether taking commonly prescribed bladder medications results in changes to the brain.
Many older women—and men—are already taking multiple anticholinergic medications, which include the most-prescribed class of bladder drugs, antimuscarinics, by the time they seek treatment for overactive bladder. Given the concerns that taking too many such medications can cause cognitive problems, Clarkson hopes to add non-pharmaceutical treatment options to the menu. “If we can keep people off the drugs, that would be great,” she says.
Causes of overactive bladder
Most researchers agree that the main obstacle to finding more effective treatments for overactive bladder syndrome is that the diagnosis is so muddy: Rather than a single disorder, it’s a loose group of symptoms that can be caused by many different conditions, from Parkinson’s disease to spinal cord injury to diabetes to none of the above. But the cases often get lumped together and talked about as if they were all the same condition, says neuroscientist Aaron Mickle of the Medical College of Wisconsin.
Mickle is studying how different conditions affect the bladder lining, the urothelium—a soft, self-renewing layer of tissue that can stretch and flatten to accommodate changes in bladder volume. Although scientists once considered the urothelium a passive barrier that renders the bladder walls leakproof, it’s now clear that it plays a key role in signaling the stretch of the bladder as it fills.
One reason that the urothelium is so sensitive is that many of its cells contain multiple types of mechanically activated ion channels—proteins that sit in cell membranes and are literally channels into the cell. When the cell membrane gets stretched, pushed or otherwise deformed, these channels open, allowing positively charged ions to flow inside the cell, explains Kate Poole, a physiologist at the University of New South Wales in Australia and author of a 2022 article in the Annual Review of Physiology on mechanically activated ion channels in mammals.
Sensory neurons that extend into the urothelium contain these force-sensing channels; when the influx of positive ions reaches a certain threshold in these nerves, they communicate directly with nerves in the spine and brain through electrical impulses. Intriguingly, however, non-neuronal cells in the urothelium also contain a variety of mechanically activated ion channels, suggesting that they, too, can signal bladder fullness.
In 2023, Mickle used optogenetics—in which the zap of a laser beam remotely activates or deactivates selected cells in animals—to selectively stimulate some of these non-neuronal urothelial cells. That was enough to activate sensory neurons and trigger bladder contractions, the first time this had been done. Eventually, Mickle hopes to develop a wireless optogenetic system that continuously monitors and modifies the activity of specific types of bladder cells in people. (Although the optogenetics technique has so far been used mainly in lab animals, researchers are now exploring its use in humans.)
Other groups are investigating as drug targets the force-sensing channels in bladder cells, as well as other channels that open in response to various nerve-signaling chemicals and hormones. These include a group of force-sensing propeller-shaped proteins called Piezo channels that play an important role in bladder sensation. In 2020, a study published in Nature showed that in addition to other profound deficits, such as difficulty walking, people with a rare mutation that affects one type of these channels, called Piezo2, struggle to sense their bladders filling. Some must pee on a set schedule or physically push down on their bladders to urinate.
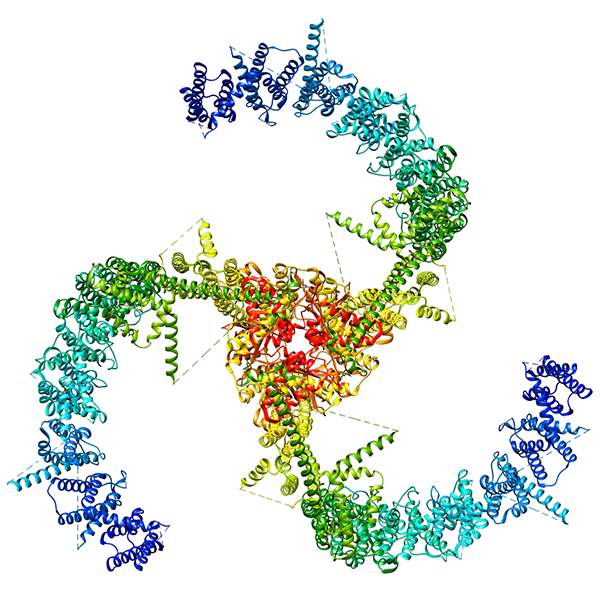
One of several types of force-sensing protein channels found in the bladder, this
three-pronged, propeller-shaped Piezo2 channel sits in the cell membrane. It opens
in response to mechanical forces such as stretch and pressure. Recently, researchers
have shown that both people and mice with genetic mutations that affect Piezo2
function have urinary deficits. These include a diminished ability to sense when the
bladder is filling or full.
GOULTARD59 / WIKIMEDIA COMMONS
Some scientists hope to target Piezo2 channels to treat a variety of bladder disorders. One advantage of targeting such channels, says Poole, is that they’re “inherently druggable,” meaning that researchers can often find small molecules that will switch them on or off even if they normally respond to mechanical stimuli.
But there’s also a downside: Like other ion channels that researchers have tried to target in the bladder, Piezo2 channels can be found all over the body, including in the lungs, joints, and heart. Consequently, any drug that affects the channels in the bladder will likely hit other parts of the body, causing safety issues. Michel points to a clinical trial for a drug that worked on another type of ion channels in the bladder—ones that let potassium ions into cells—but had to be discontinued because it turned out to cause liver problems.
There is at least one way to overcome that obstacle, at least in theory: gene therapies that specifically target bladder tissue because they’ve been directly injected into the detrusor muscle or have been infused via catheter into the urethra. In 2023, scientists published preliminary but encouraging data from a clinical trial with 67 patients of a genetic therapy that targets the bladder’s potassium channels.
Although scientists who focus on the bladder and urinary tract have traditionally worked separately from those researching the spinal cord and brain, these long-siloed fields are starting to link up and collaborate, putting more pieces of the brain-bladder puzzle together. Mickle, for example, has recently teamed up with a neuroimaging lab that will help him observe how a mouse’s brain responds to optogenetic stimulation of its urothelial cells.
In the past, “we never focused on the brain,” Valentino says. But the new research, she says, “is allowing us to think more about these other targets.”
Source
Hope you enjoyed this news post.
Sincere thank you for your Feedback and Likes.

3175x175(CURRENT).thumb.jpg.b05acc060982b36f5891ba728e6d953c.jpg)
Recommended Comments
There are no comments to display.
Join the conversation
You can post now and register later. If you have an account, sign in now to post with your account.
Note: Your post will require moderator approval before it will be visible.